Ask anything about research
Search papers, query evidence, get expert commentary — all in one place
ACC 2026 Late-Breaking Trials
Live trial results, expert commentary, and discussion with 10+ trial authors
Research Pulse
Hot Research Today
Papers from every journal, all in one place
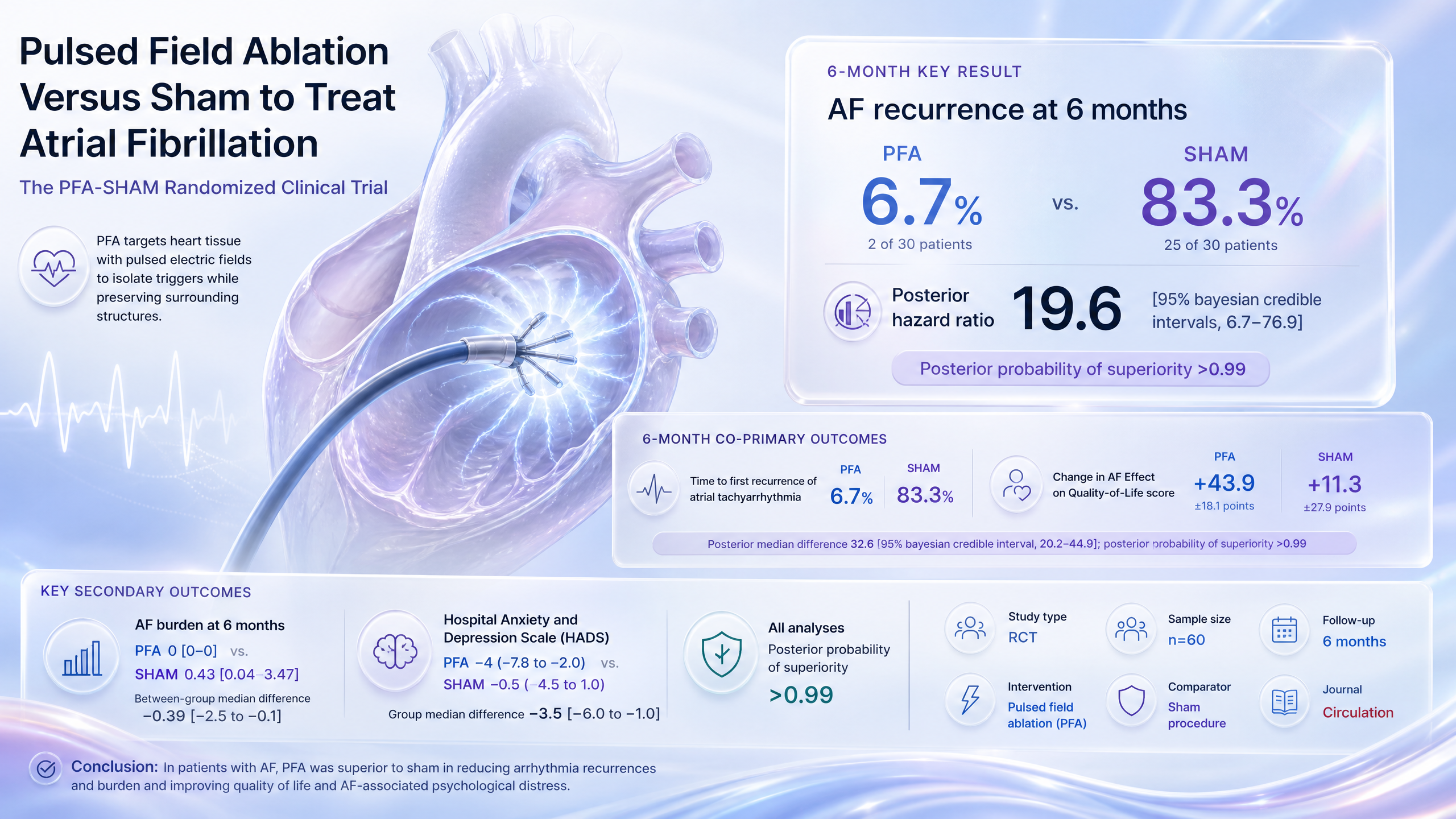
Pulsed Field Ablation Versus Sham to Treat Atrial Fibrillation: The PFA-SHAM Randomized Clinical Trial
Pulsed field ablation cuts 6-month atrial tachyarrhythmia recurrence by ~92% versus sham.
Implication: PFA markedly outperforms sham for AF recurrence and QoL; confirms ablation benefit beyond placebo in symptomatic patients.
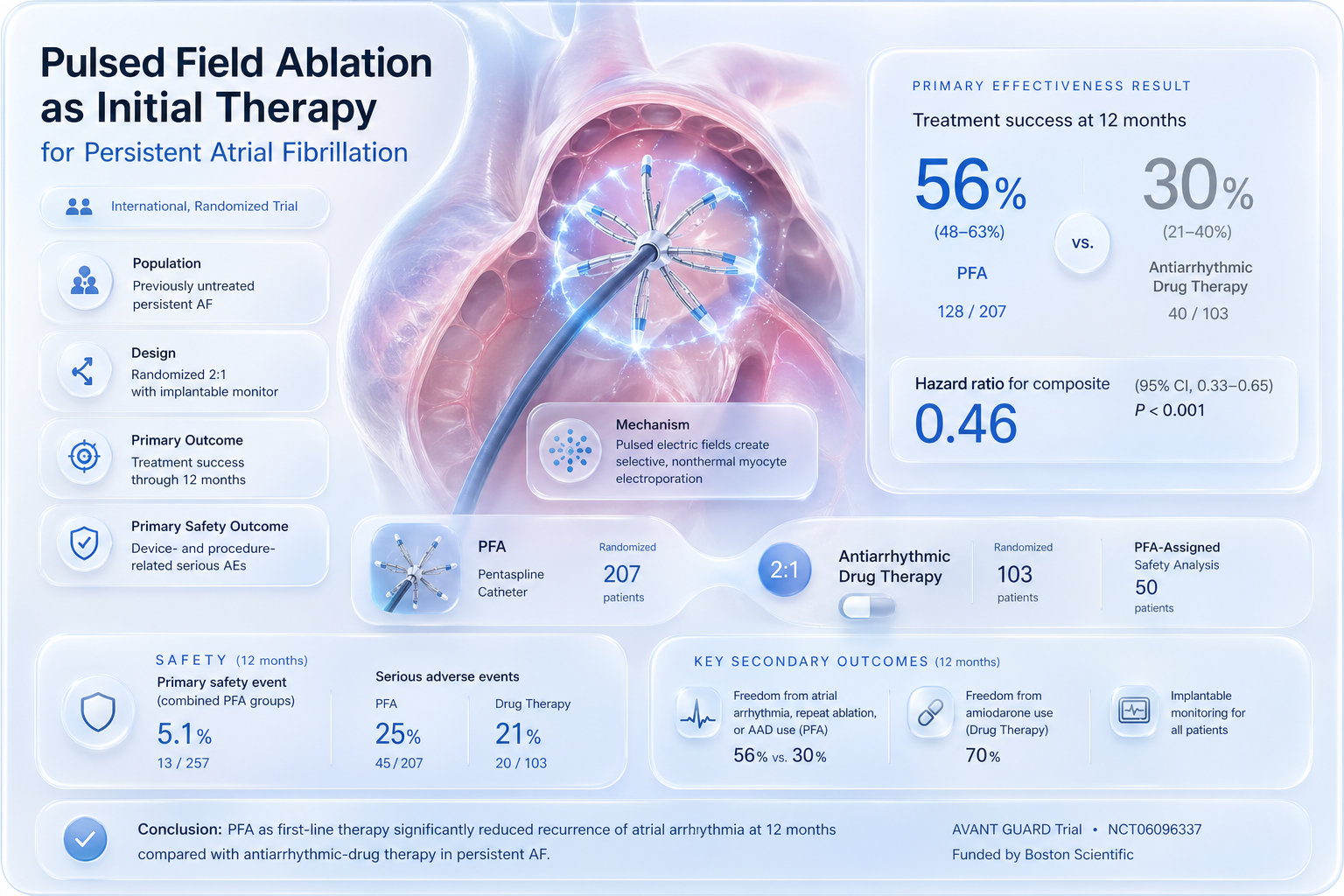
Pulsed Field Ablation as Initial Therapy for Persistent Atrial Fibrillation
Initial PFA cuts composite treatment failure ~54% vs. antiarrhythmic drugs in persistent AF.
Implication: Supports first-line PFA over AADs in persistent AF; challenges guidelines mandating drug trial first and extends paroxysmal AF evidence.
“These findings have implications for clinical practice, for guidelines, and for insurance coverage because “there’s a lot of people that are dissuading us from doing persistents because it’s lower yield,” Tung said.”
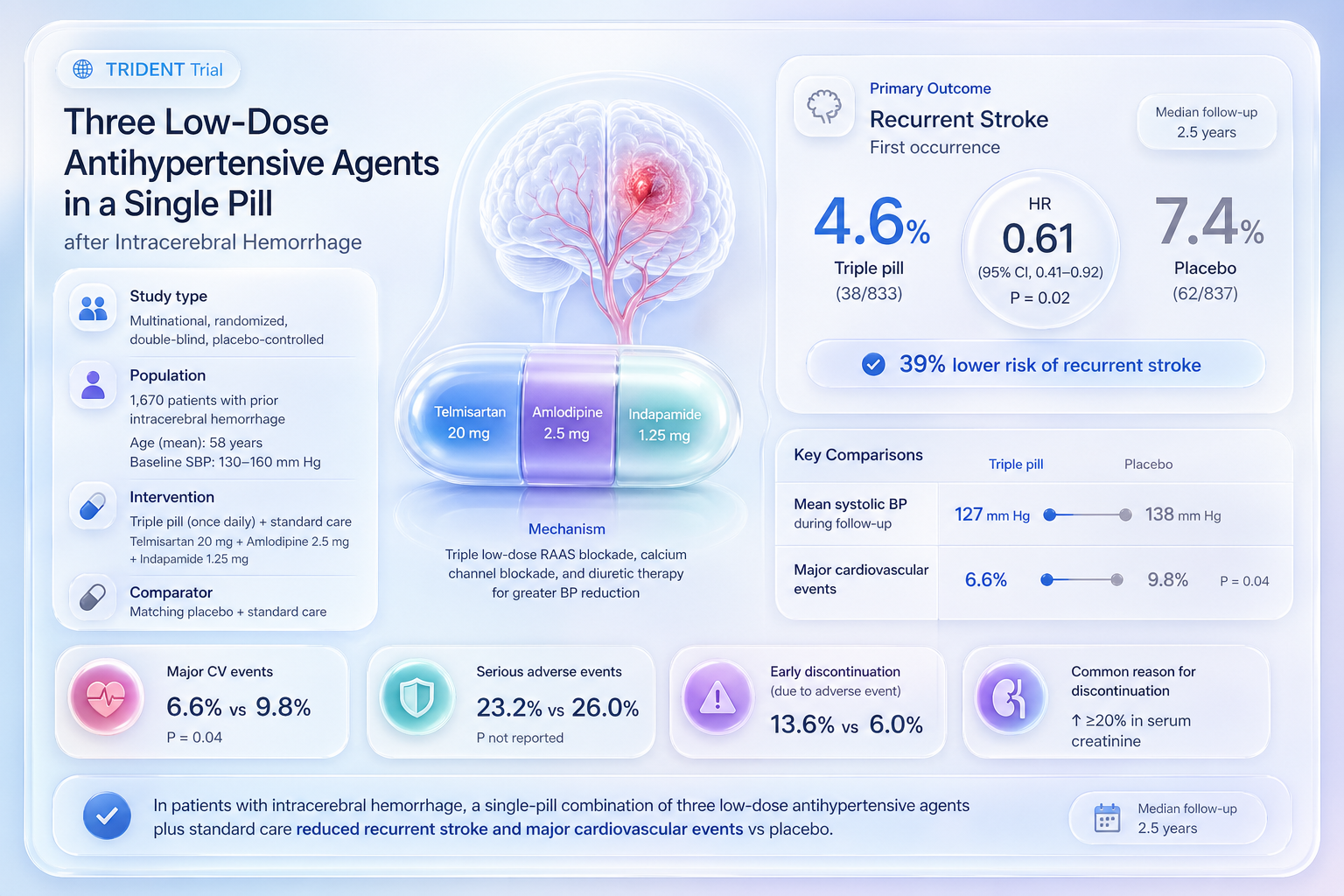
Three Low-Dose Antihypertensive Agents in a Single Pill after Intracerebral Hemorrhage
Low-dose triple antihypertensive pill cuts recurrent stroke ~39% versus placebo.
Implication: Supports single low-dose triple pill after ICH for better BP control; extends INTERACT evidence with practical adherence-enhancing approach.
“Meaningful blood pressure control after intracerebral hemorrhage requires a coordinated, systemwide commitment that integrates team-based care, expanded access to medication, and real-time monitoring to bridge the gap between clinic visits and daily management. Beyond the primary care office, eve...”
Role of Physical Activity in Obesity Treatment and Cardiometabolic Health: A Scientific Statement From the American Heart Association
Implication: Prescribe physical activity for cardiometabolic gains irrespective of weight loss; extends evidence for multimodal obesity management.

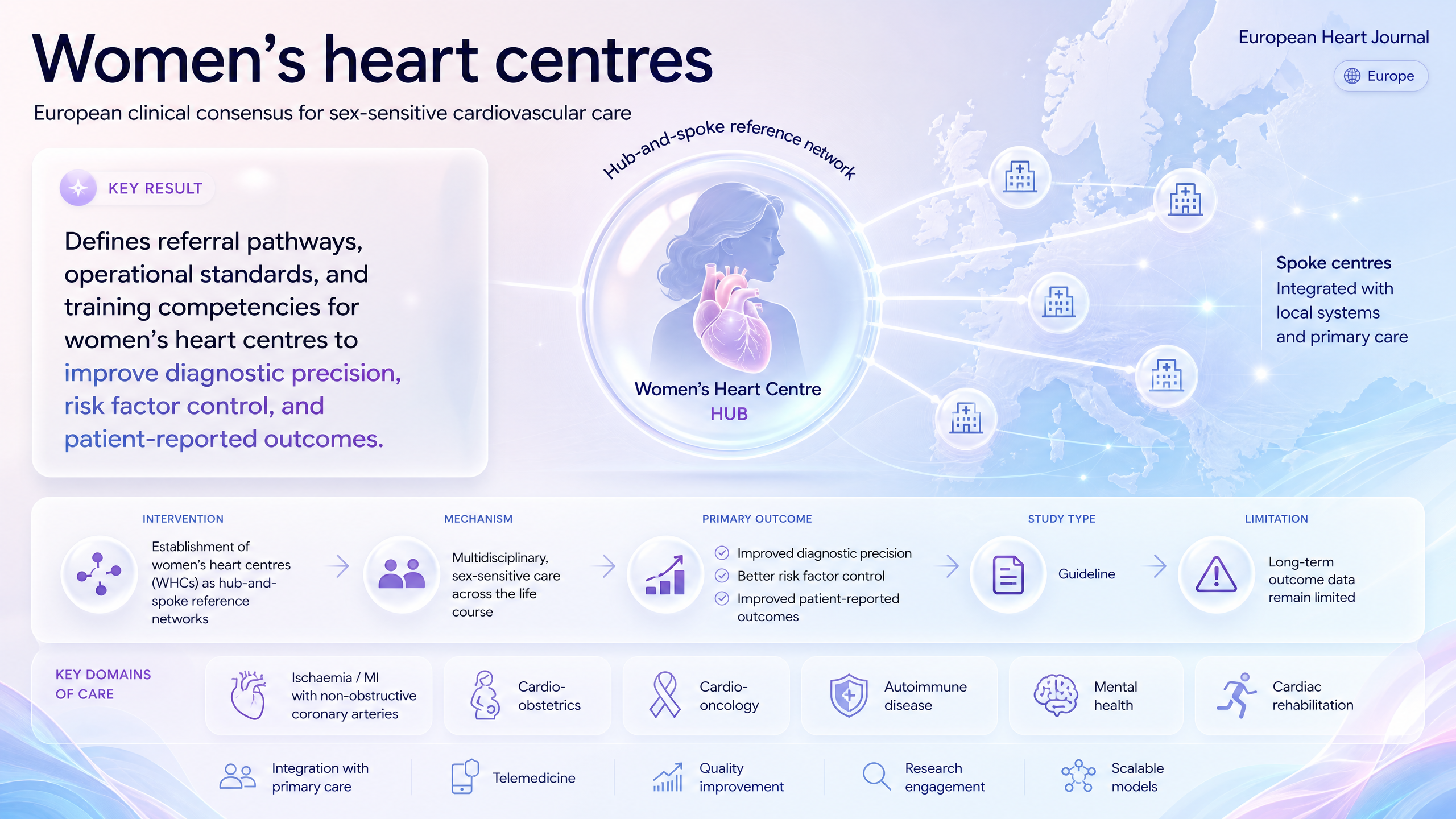
Women's heart centres: a clinical consensus statement of the European Association of Cardiovascular Imaging (EACVI), the European Association of Percutaneous Cardiovascular Interventions (EAPCI), the Heart Failure Association (HFA), and the Association for Acute CardioVascular Care (ACVC) of the ESC
Implication: Supports women's heart centre implementation to reduce sex-based care gaps; extends consensus on specialized pathways and training.
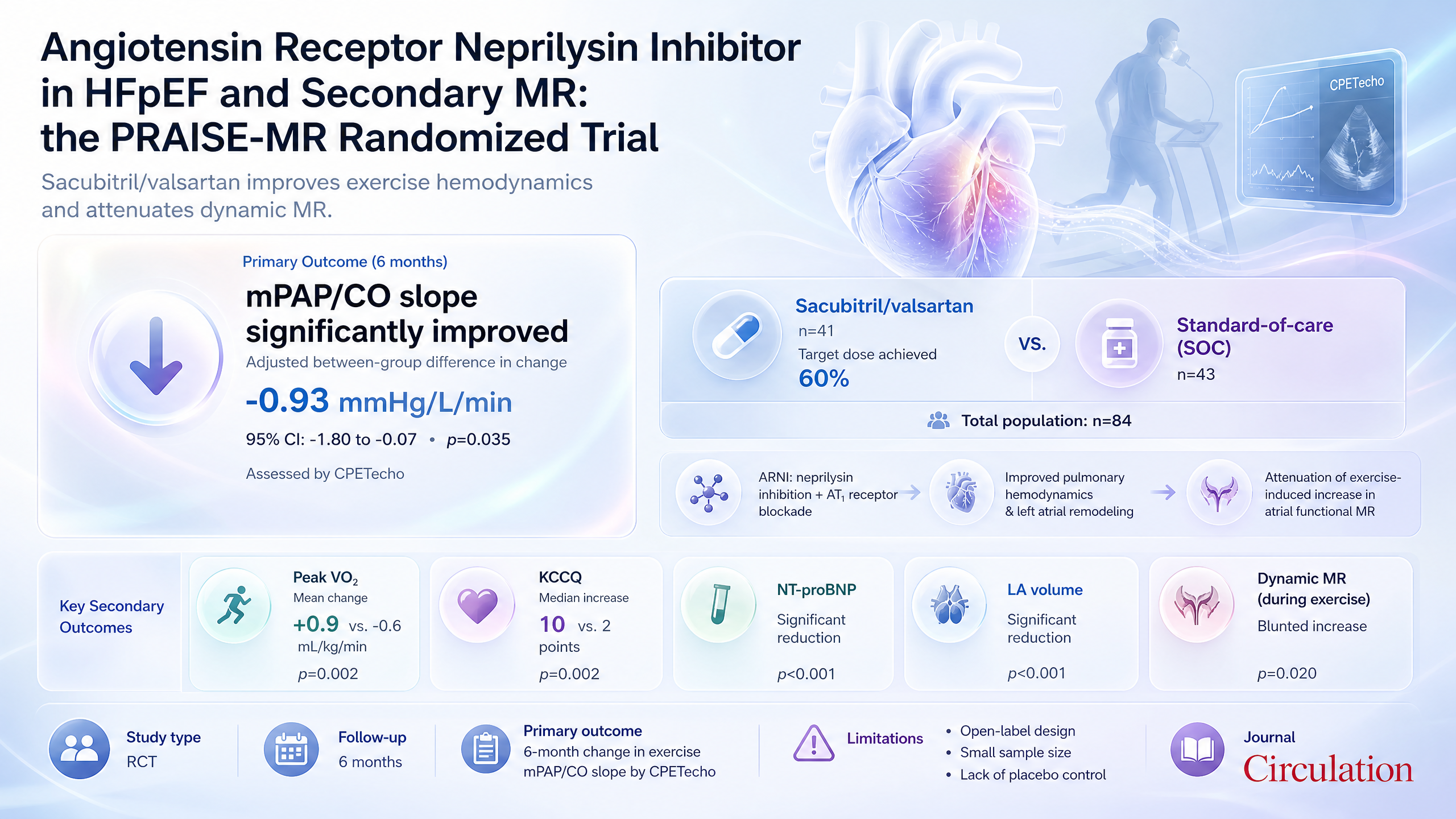
Angiotensin Receptor Neprilysin Inhibitor in Heart Failure with Preserved Ejection Fraction and Secondary Mitral Regurgitation: the PRAISE-MR Randomized Trial
Sacubitril/valsartan improves exercise mPAP/CO slope by ~0.93 mmHg/L/min versus SOC in HFpEF with AFMR.
Implication: Supports sacubitril/valsartan over SOC in HF with adverse exercise hemodynamics; extends prior ARNI trials to this invasive endpoint.
“The PRAISE-MR trial is the first prospectively randomized trial to demonstrate that sacubitril/valsartan significantly improves exercise hemodynamics, functional capacity, and quality of life in patients with HFpEF and AFMR. These findings underscore that the phenotypic heterogeneity of HFpEF nec...”
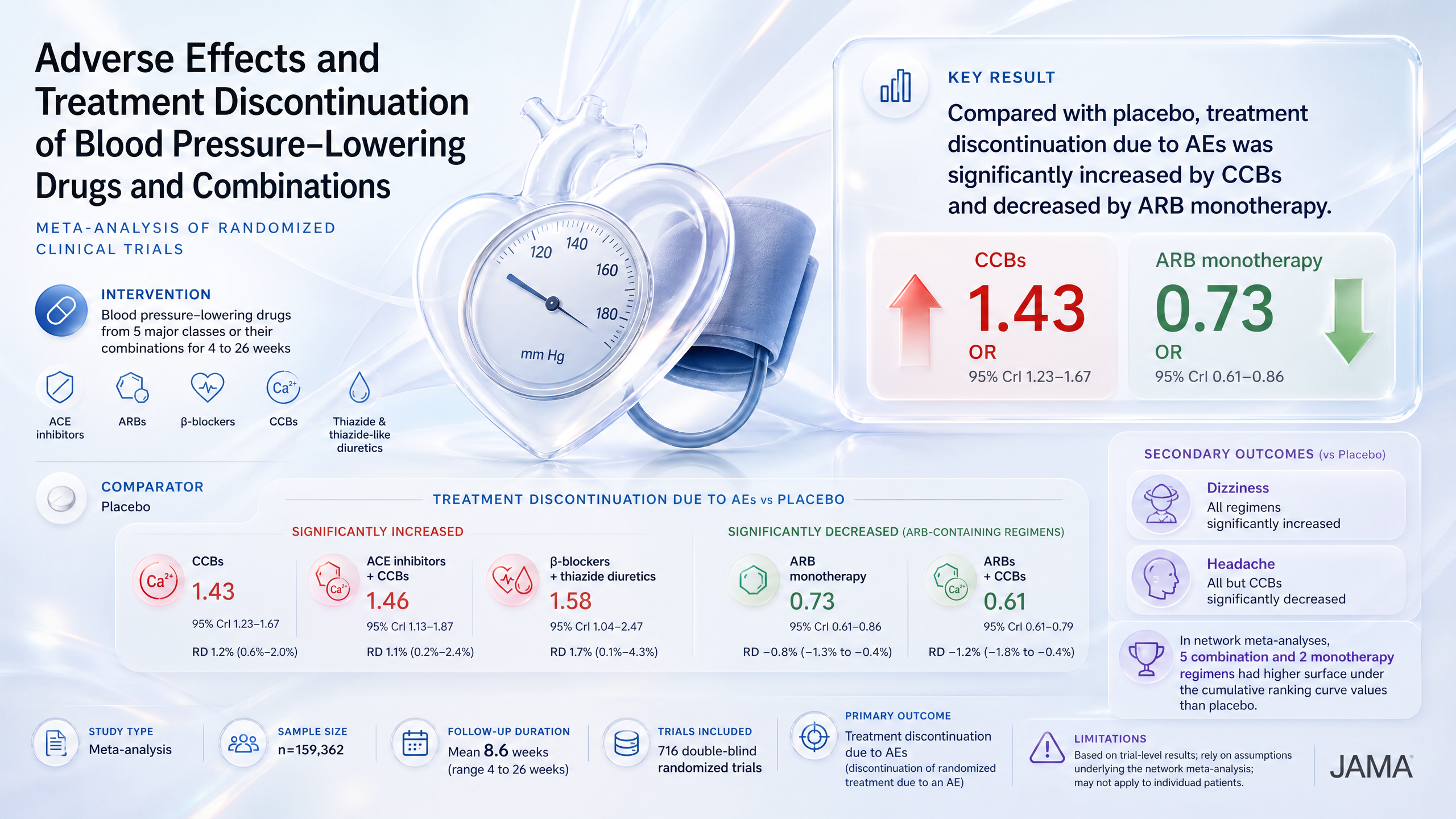
Adverse Effects and Treatment Discontinuation of Blood Pressure–Lowering Drugs and Combinations
CCBs increase adverse event discontinuations ~43% versus placebo while ARB monotherapy reduces them.
Implication: Adverse effects leading to discontinuation vary significantly by antihypertensive class, with ARB-containing regimens showing fewer withdrawals than placebo, suggesting better overall tolerability.
“Results from the study by Wang, et al., can help inform clinicians' selection of antihypertensive therapies for patients initiating medications for hypertension, particularly when comorbidities, such as the presence of diabetes with microvascular disease, do not warrant a specific therapy.”
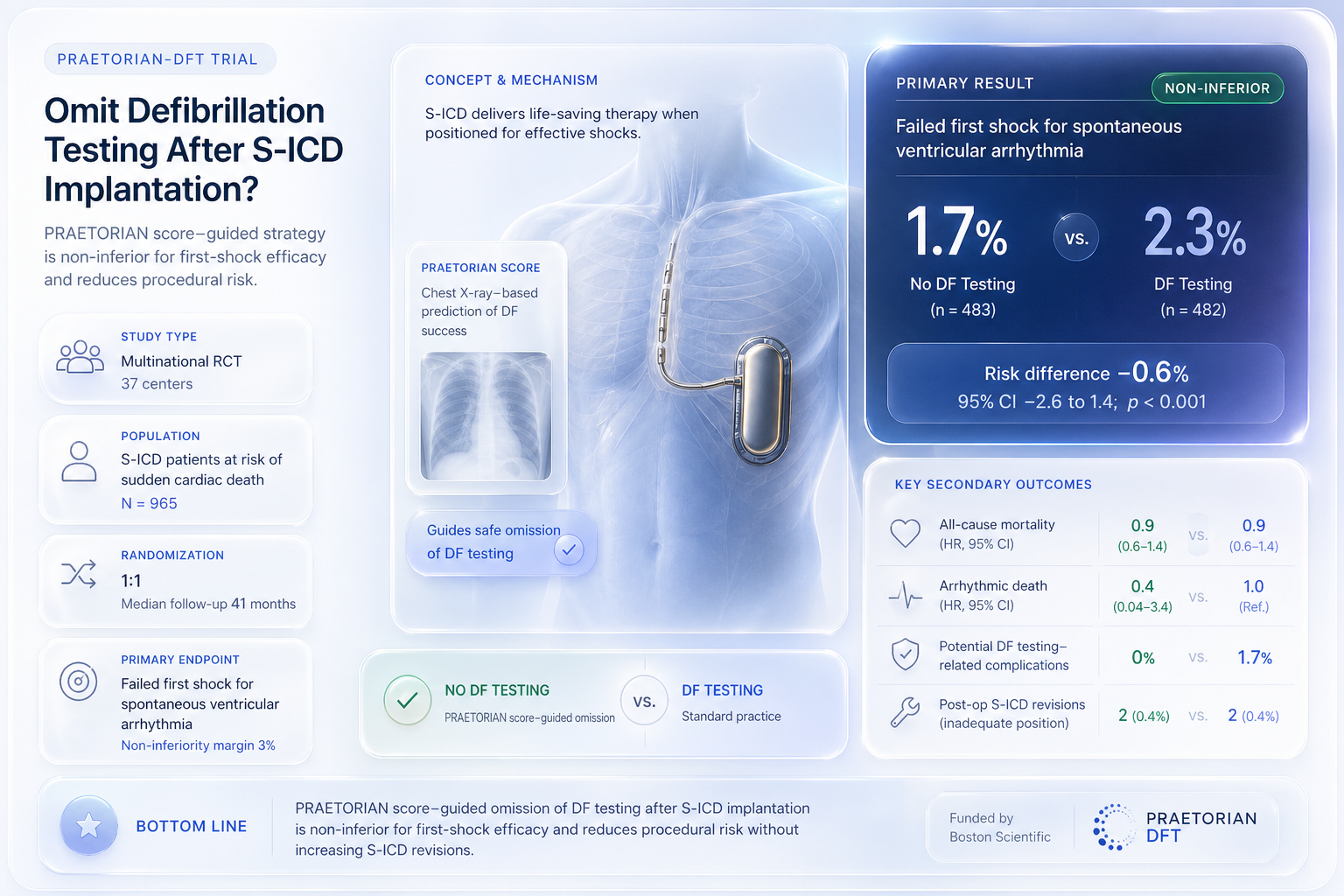
Subcutaneous Defibrillator Implantation With or Without Defibrillation Test: The Primary Results of the Randomized PRAETORIAN-DFT Trial
PRAETORIAN score-guided omission of defibrillation testing is non-inferior to routine testing for failed first shocks.
Implication: Supports PRAETORIAN-guided omission of routine DFT in S-ICD patients; confirms non-inferior efficacy and reduced procedural risk.
“The risk-benefit ratio of routinely performing DT seems to favor not doing routine testing.”
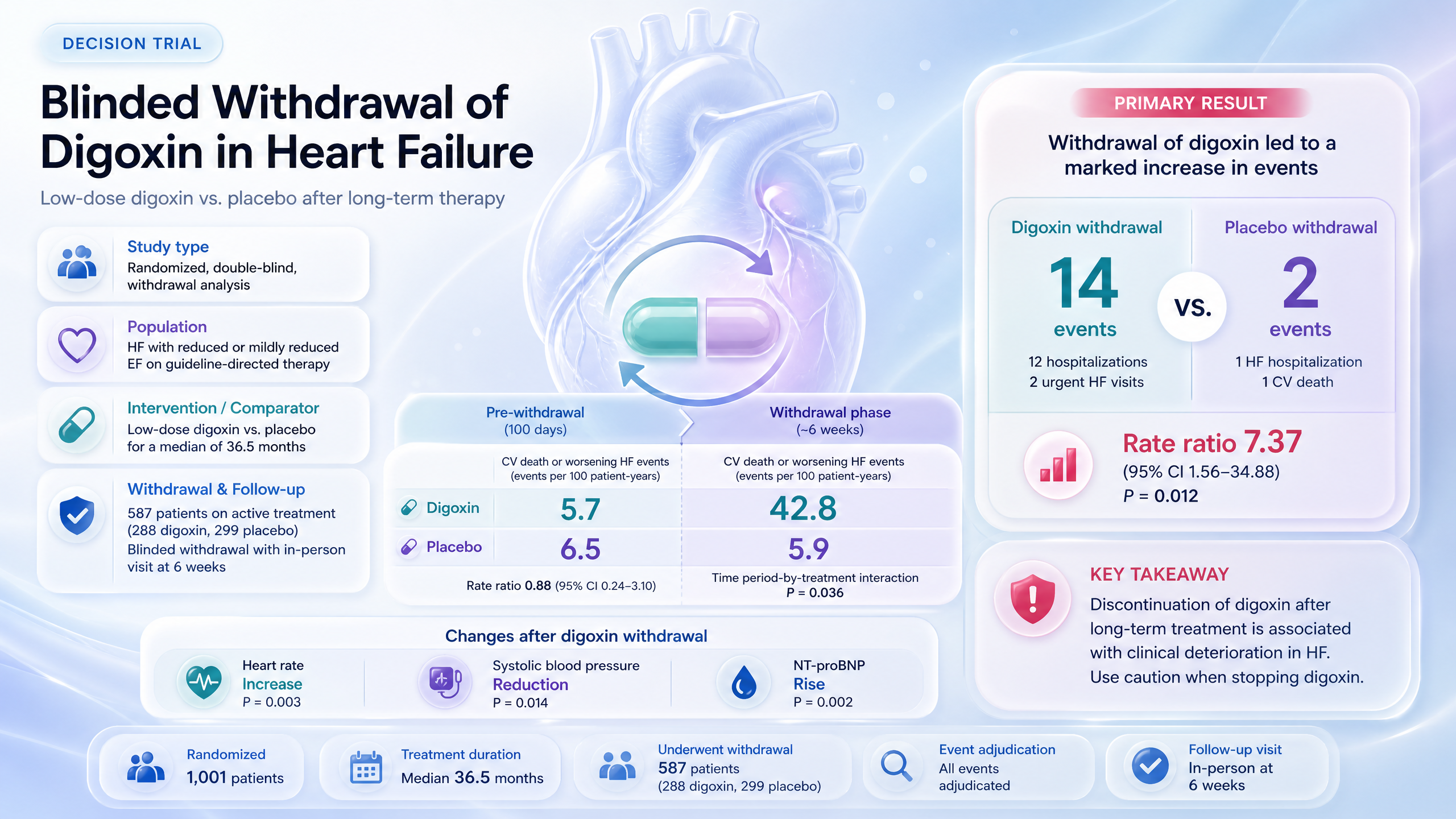
Blinded withdrawal of randomized treatment with low-dose digoxin or placebo in patients with heart failure: the DECISION trial
Withdrawing low-dose digoxin increases CV death or worsening HF events ~637% vs placebo.
Implication: Caution against digoxin withdrawal in stable HF; confirms ongoing benefit of continued therapy.
“Discontinuation of long-term low-dose digoxin is associated with clinical deterioration of patients with chronic [HF] and a [LVEF] <50%. These findings warrant caution when stopping low-dose digoxin.”
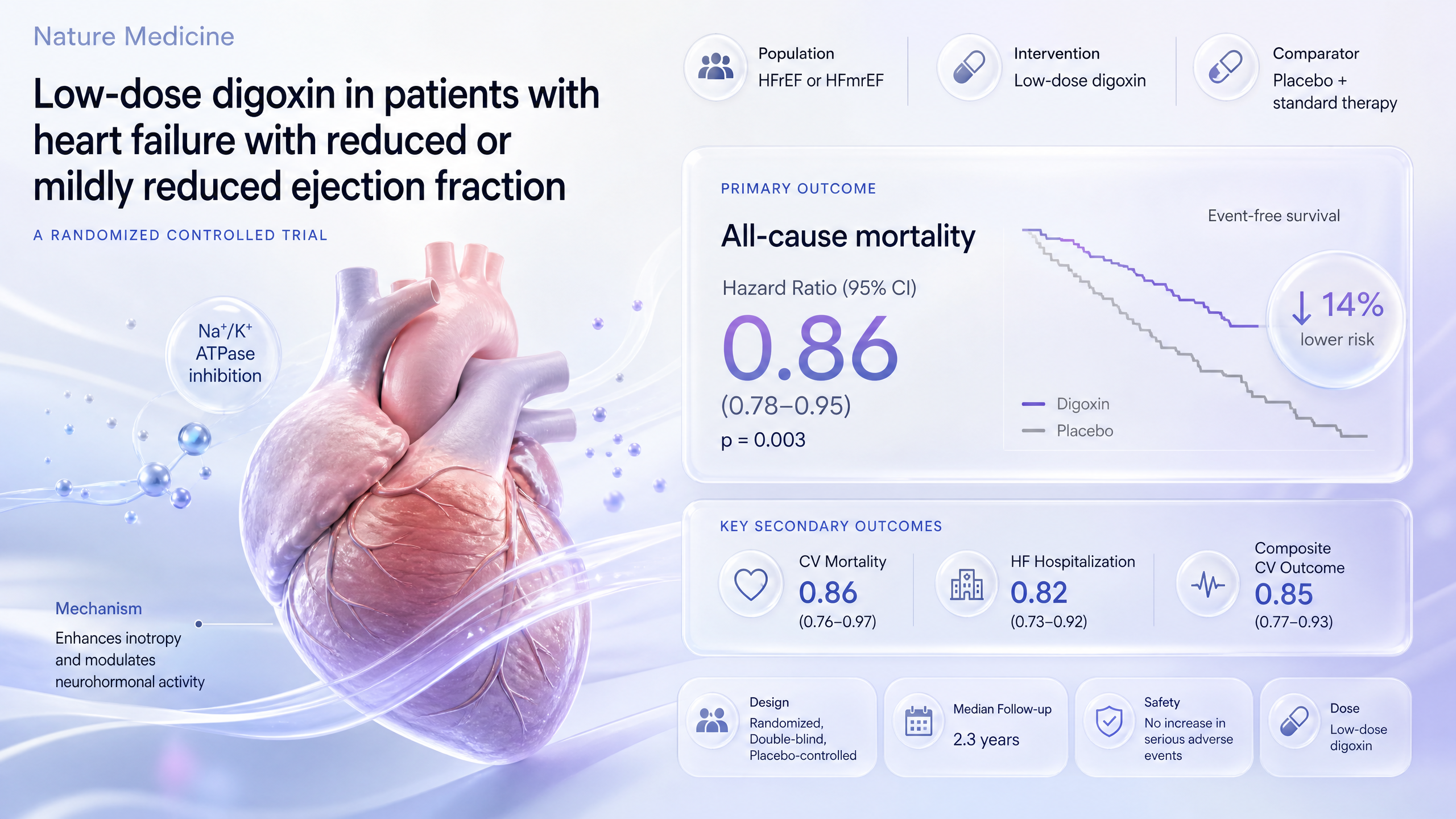
Low-dose digoxin in patients with heart failure with reduced or mildly reduced ejection fraction: a randomized controlled trial
Low-dose digoxin fails to reduce worsening heart failure or cardiovascular mortality compared to placebo.
Implication: Does not support routine low-dose digoxin use in HFrEF or HFmrEF; leaves open class effects and secondary benefits for further study.
“the results will determine whether the reevaluation applies to all members of this therapeutic class or only to digitoxin”